Evolution® Kinematic Alignment Technique
Match your patient’s natural knee anatomy by combining the latest kinematic alignment technique with the patient-preferred Medial-Pivot knee design.1
Over 25 years ago, MicroPort established the Medial-Pivot Knee design that replicates the natural stability and motion of the knee, while also delivering a functionally-restorative design that offers surgeons an innovative solution to problems such as instability, anterior knee pain, and functional limitations. Now, we’re continuing to innovate total knee replacements with the latest addition of our Kinematic Alignment (KA) technique.
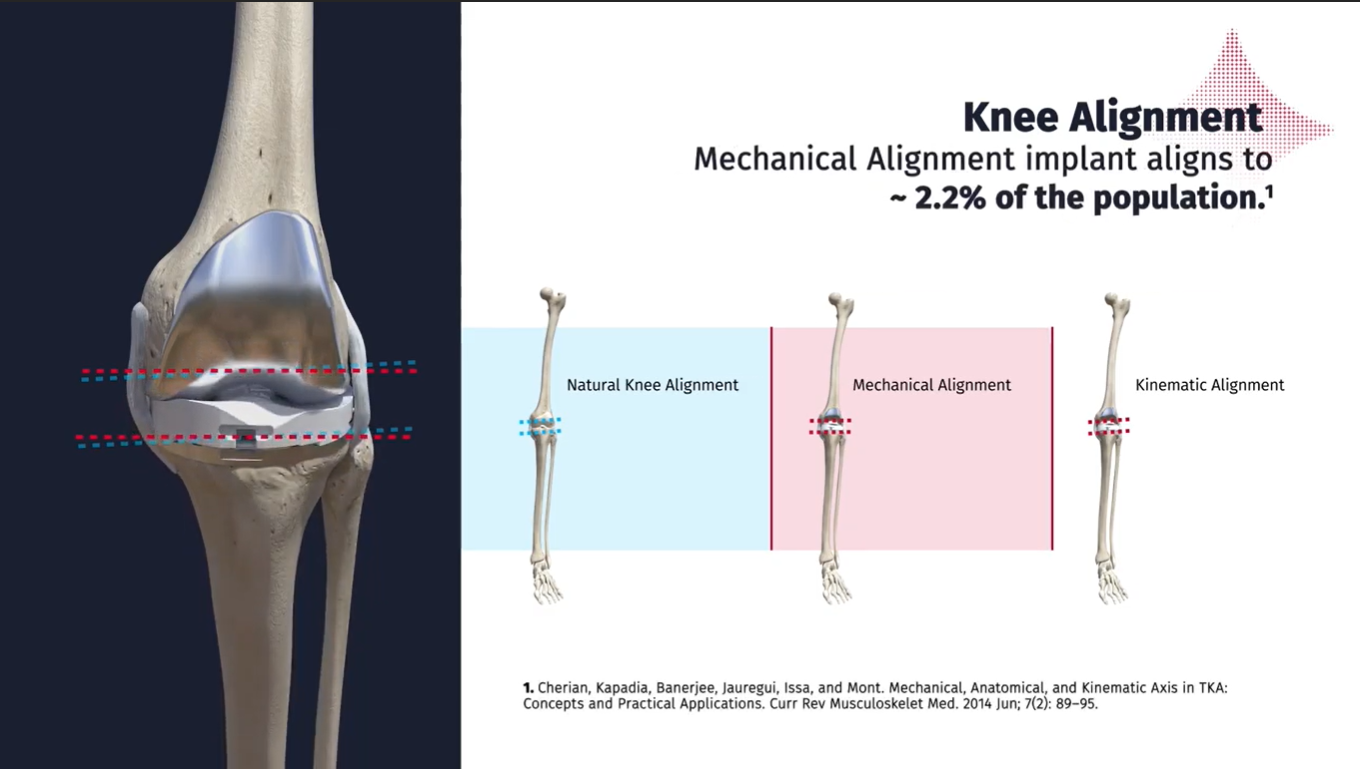
The Kinematic Alignment surgical technique allows surgeons to duplicate the pre-arthritic native joint line of their patient, as opposed to the more traditional Mechanical Alignment (MA) technique that ignores each patient’s individual anatomy by utilizing non-anatomic cuts. The Mechanical Alignment technique works. However, approximately 20% of knee replacement patients remain unsatisfied with their total knee replacement.2 MicroPort’s Kinematic Alignment technique, combined with the Medial-Pivot design philosophy, strives to address this dissatisfaction which can arise due to instability, stiffness, pain, or a patient’s inability to perform at a high level.2,3,4
Learn how the benefits of Medial-Pivot kinematics and the Kinematic Alignment technique combine to individualize the knee implantation for each patient.5,6 Download our brochure to learn more:
An optimal total knee surgery should be accomplished with minimal resections and releases. The MicroPort Kinematic Alignment technique utilizes mechanical instruments and the “Measure Twice, Cut Once” methodology to restore your patient’s natural anatomy through repeated intra-operative measurement and limited guesswork. By prioritizing the pre-arthritic femoral joint line, and directly tying the tibial resection to the femoral resection through native ligament tension, little to no bony re-cuts or ligament releases are required.
These surgeons are paid consultants for MicroPort Orthopedics. The opinions expressed are theirs alone and do not necessarily reflect the opinions of MicroPort Orthopedics Inc.
MicroPort Orthopedics is driven to meet the growing needs of patients, surgeons, and payors to better manage a patient’s episode of care with improved outcomes, less rehabilitation requirements, and reduced post-op restrictions.
